
Effectiveness
Another principal benefit of Limbrel is that it provides effective management of the metabolic processes of osteoarthritis. Limbrel's effectiveness comes from:
Unique Dual Inhibition Mechanism of Action via Dietary Management
Antioxidant Activity
Clinical Experience
Unique Dual Inhibition Mechanism of Action via Dietary Management
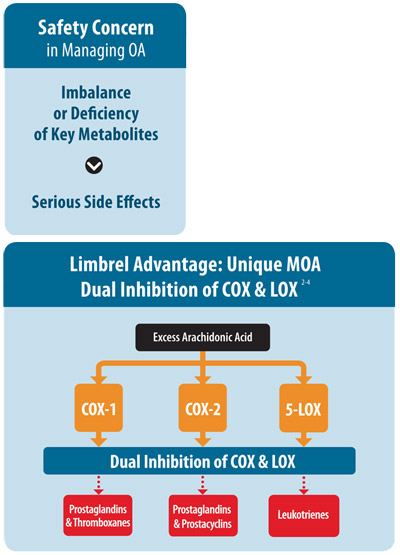 After the initial damage to joints, osteoarthritis progression is largely due to excess arachidonic acid (AA) metabolism on both COX (cyclooxygenase) and LOX (lipoxygenase) pathways (1-2).
After the initial damage to joints, osteoarthritis progression is largely due to excess arachidonic acid (AA) metabolism on both COX (cyclooxygenase) and LOX (lipoxygenase) pathways (1-2).
Limbrel’s approach for the dietary management of osteoarthritis is very different from other osteoarthritis products. Limbrel does not treat or mask the symptoms of osteoarthritis, but rather works by managing the underlying metabolic processes, which lead to as well as cause progression of the disease. Limbrel is designed to help restore the homeostasis of metabolic processes that are associated with osteoarthritis through dietary management. Limbrel manages the metabolic processes of osteoarthritis via a dual inhibition mechanism of action down both COX and LOX pathways providing highly demanded safety and effectiveness.
Implications of the inflammatory response in the LOX pathway is not widely-known:- Both LOX and COX pathways convert AA into inflammatory mediators that, if chronically produced, can lead to progression of osteoarthritis (3-4).
- When either COX-1 or COX-2 or both enzymes are down-regulated, AA metabolism is shunted down the LOX pathway to generate inflammatory metabolites (5).
- The 5-LOX enzyme converts AA into an inflammatory mediator called leukotriene B4 (LTB4) that causes cell and fluid buildup in osteoarthritis joints (6-7).
- LTB4 acts as strong chemotactic attractants of white blood cells (WBC) to the site of injury (8). This can occur anywhere in the body including damaged joints.
- When traditional NSAIDs down-regulate prostaglandins required for maintenance of stomach mucosa, 5-LOX is up-regulated in the stomach mucosa converting AA to LTB4. This process is normally necessary for tissue repair. In the stomach, however, WBCs are attracted to the mucosa causing an increase in inflammation which contributes to ulceration (2, 9-10).
- Metabolism of AA in the COX pathway and inhibition of this process with traditional NSAIDs or selective COX-2 inhibitors affects metabolism of AA in the LOX pathway. COX inhibitors increase the production of LOX based inflammation both in the gastric and joint tissue (2, 5).
- Management of LOX pathway metabolism is essential in the dietary management of osteoarthritis.
- Metabolism of AA by COX-1 generates prostaglandins important for the preservation of stomach mucosa and thromboxanes for platelet function as well as vasoconstriction in vessels (11).
- Metabolism of AA by COX-2 generates prostacyclins, which is required for vasodilation of vessels, antagonistic to thromboxanes and prostaglandins involved in tissue repair (11).
- If COX-1 is selectively targeted, prostaglandins production in the stomach decreases, there is an increased incidence of ulceration (9-10).
- If COX-2 is selectively targeted, prostacyclins production decreases. Thromboxanes then dominate causing vasoconstriction of the arterioles in the kidney reducing urine output leading to elevated systolic blood pressure and peripheral edema (12). In extreme cases, this imbalance can cause a prothrombotic event which can result in a heart attack or stroke (13).
- Thus, balanced management of both COX-1 and COX-2 is crucial for the dietary management of osteoarthritis.
With a balanced inhibition of COX-1 & COX-2, and the dual inhibition of COX & LOX, Limbrel dampens inflammation through its clinical dietary management of the metabolic aspects of osteoarthritis. Unique flavonoid ingredients in Limbrel are the key for exceptional safety and effectiveness in managing the metabolic processes of osteoarthritis.
Antioxidant Activity
Limbrel is a powerful antioxidant, which "soaks up" free radicals. Free radicals are also known as oxidative products, which are collectively called reactive oxygen species (ROS). ROS contribute to the breakdown of synovial tissue, and induce the pro-inflammatory protein signals that lead to cartilage degradation in osteoarthritis.
ROS generated by WBC influx into the joint cause increased production of the transcription factor NFκB at the cellular level which induces the production of pro-inflammatory cytokines such as TNFα which in turn induces IL-6 (14). TNFα, along with IL-1β and IL-6, are the initial signals that induce further expression of 5-LOX and COX-2 in osteoarthritis (15).
Limbrel has an antioxidant ORAC (Oxygen Radical Absorbency Capacity) score is 5517 umole TE/g, higher than Vitamin C and E (16). By reducing these key cytokines on a cellular level, via this antioxidant mechanism, Limbrel manages the production of excess inflammatory metabolites which contribute to osteoarthritis. Therefore, Limbrel's antioxidant capacity may reduce oxidative stress and minimize further cartilage damage caused over time by ROS produced by the action of WBCs or environmental influences.
Clinical Experience
Double-blind, Randomized Clinical Study vs. Naproxen§
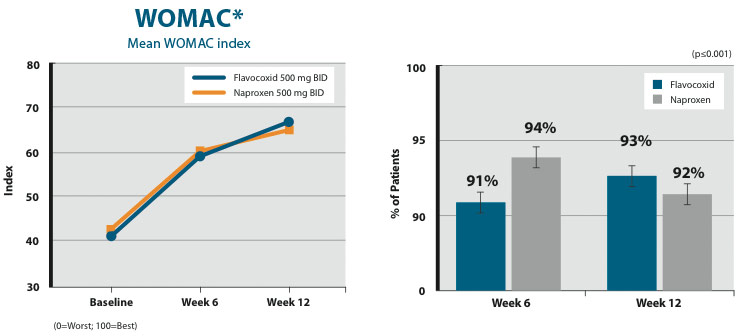
LIMBREL was evaluated in a double-blind, randomized, active comparator (naproxen) controlled clinical study that enrolled 103 subjects with moderate or moderate-severe OA of the knee. Subjects were randomly assigned to receive either LIMBREL (500 mg BID) or naproxen (500 mg BID) for 4 weeks. Primary endpoints were the short WOMAC composite index (Western Ontario and McMaster Universities Osteoarthritis Index), investigator VAS for global response, subject VAS scales for global response and discomfort. Subjects were sex-matched and recruited from ages 35 to 85 years with an average age of 57-60 years per arm. There were no differences in demographic characteristics or in baseline WOMAC or VAS scores between the two arms. Subjects taking NSAIDs and/or gastroprotective medication underwent a 2-week washout period before beginning the trial. Subject activity was not restricted, and subjects were free to withdraw from the trial at any time for any reason. Dropouts were minimal in both arms. Two subjects, one from each arm, failed to complete the trial for personal reasons unrelated to the study.
In this study, both LIMBREL and naproxen arms noted significant reduction in the signs and symptoms of knee OA. All within-arm improvements in efficacy endpoints were statistically significant (p≤0.001). The LIMBREL and naproxen arms performed nearly identically, and the between group differences were not statistically significant for any efficacy endpoint. See Figures 1-4 below for efficacy results of LIMBREL vs. naproxen in this study.
§ Levy R, Saikovsky R, Shmidt E, Khokhlov A. Safety, efficacy and acceptability of flavocoxid (Limbrel™) compared with naproxen in subjects with osteoarthritis of the knee: a pilot study. Osteoarthritis and Cartilage. 2007; 15(suppl B):B91
Figure 1. Improvement in WOMAC*
Figure 2. Improvement in Physician VAS
(Global Disease Assessment)**
Figure 3. Improvement in Subject VAS
(Global Disease Assessment)
Figure 4. Improvement in Subject VAS
(Discomfort Assessment) 
Fisher's exact test was computed for improved vs. not improved (sum of unchanged and worsened) for all parameters (see Table 1). Both arms had a large percentage of subjects with significant improvement (75% to 88%). Differences were not significant between arms for percent of patients with improvement. There was a slight, non-significant trend toward greater improvement in physician global disease assessment VAS in the LIMBREL arm and WOMAC in the naproxen arm.
| LIMBREL 500 mg BID (N=52) | Naproxen 500 mg BID (N=51) | p-value | |
| WOMAC | 79% | 88% | < 0.001 |
| Physician VAS (global disease assessment) | 83% | 75% | < 0.001 |
| Subject VAS (global disease assessment) | 87% | 88% | < 0.001 |
| Subject VAS (discomfort assessment) | 87% | 88% | ≤0.001 |
Safety of flavocoxid vs. placebo ¥
This study was designed to determine the safety of flavocoxid (Limbrel) in the management of knee osteoarthritis. The 12-week, randomized, double-blind, placebo-controlled trial in an academic medical center enrolled 59 patients with moderate osteoarthritis of at least one knee who were classified as having ''below average'' to ''a moderately above average cardiovascular risk'' with a Framingham-based scoring tool. Subjects were randomized to flavocoxid 250 mg twice a day versus identical placebo. Safety measures, including recording of adverse events, incidence of serious adverse events, and results of routine laboratory values, were compared between the two groups. There were no major differences in the baseline demographic characteristics of the placebo and flavocoxid groups. With one exception, no significant differences were found between the two groups with respect to adverse events by body system, blood pressure, or laboratory values. This difference was a significantly higher incidence of ear nose and throat and upper respiratory adverse events in the placebo group (35.4%) vs. flavocoxid (5.8%, p=0.0003). There were no intra- or inter-group differences in any of the laboratory parameters from study baseline to completion.
¥ Morgan S, Baggott J, Moreland L, Desmond R, Kendrach A. The safety of flavocoxid, a medical food, in the dietary management of knee osteoarthritis. J Med Food. 2009;12 (5)1143-1148
| Body system | Flavocoxid (n = 52 events) |
Placebo (n = 48 events) |
Fisher's exact test (two-tail) P value |
| Cardiovascular | 0 (0.0%) | 1 (2.1%) | .48 |
| Constitutional | 5 (9.6%) | 1 (2.1%) | .21 |
| Skin | 3 (5.8%) | 0 (0.0%) | .24 |
| Ear, nose and throat | 2 (3.8%) | 12 (25.0%) | .003 |
| Pulmonary | 1 (1.9%) | 5 (10.4%) | .10 |
| Ear, nose, and throat and pulmonary | 3 (5.8%) | 17 (35.4%) | .0003 |
| Gastrointestinal | 13 (25.0%) | 12 (25.0%) | 1.0000 |
| Genitourinary | 1 (1.9%) | 2 (4.2%) | .61 |
| Musculoskeletal | 19 (36.5%) | 12 (25.0%) | .28 |
| Neurological | 7 (13.5%) | 2 (4.2%) | .16 |
| No adverse events* | 9 (30%) | 9 (31%) | 1.0000 |
| *The denominator for the percentage of no adverse events is the number of subjects. | |||
3-month comparison of full therapeutic doses of Limbrel vs. naproxen. ¶
This study was designed to compare the effectiveness and safety of flavocoxid to naproxen in subjects with moderate to severe osteoarthritis (OA) of the knee. In this randomized, multicenter, double-blind study, 220 subjects were assigned to receive either Limbrel (500 mg twice daily) or naproxen (500 mg twice daily) for 12 weeks. The trial was structured to show non-inferiority of Limbrel (flavocoxid) to naproxen. Primary outcome measures included the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) and subscales and a timed walk. Results: More than 90% of the subjects in both groups noted significant reduction in the signs and symptoms of knee OA at 6 and 12 weeks. There were no statistically significant differences in efficacy between the flavocoxid and naproxen groups when the entire intent-to-treat population was analyzed. The flavocoxid group had significantly fewer upper gastrointestinal (UGI) and renal (edema) adverse events (AEs) as well as a strong trend toward fewer respiratory AEs. Flavocoxid was as effective as naproxen in managing the signs and symptoms of OA of the knee and demonstrated better UGI, renal (edema), and respiratory safety profiles than naproxen.
¶ Levy R, Khokhlov A, Kopenkin S, Bart B, Ermolova T, Kantemirova R, Mazurov V, Bell M, Caldron P, Pillai L, Burnett BP. Efficacy and safety of flavocoxid, a novel therapeutic, compared with naproxen: a randomized multicenter controlled trial in subjects with osteoarthritis of the knee. Advances in Therapy. 2010; 27:731-42
| Adverse events | Flavocoxid (n=106) |
Naproxen (n=114) |
P value |
| Edema (no. of episodes) | 2 | 13 | 0.016 |
| Dyspepsia | 11 | 24 | 0.041 |
| Flatulence | 4 | 1 | 0.042 |
| Body as a whole | 4 | 9 | 0.070 |
| Constipation | 0 | 4 | 0.120 |
| Respiratory | 9 | 17 | 0.150 |
3-month comparison of full therapeutic doses of Limbrel vs. naproxen, a subanalysis #
Twice-daily Limbrel (flavocoxid) was evaluated for 12 weeks in a randomized, double-blind, active-comparator study against naproxen in 220 subjects with moderate-severe osteoarthritis (OA) of the knee. As described above, both groups noted a significant reduction in the signs and symptoms of OA with no detectable differences in efficacy between the groups when the entire intent-to-treat population was considered. This post-hoc analysis compared the efficacy of Flavocoxid to naproxen in different subsets of patients, specifically those related to age, gender, and disease severity as reported at baseline for individual response parameters. In this subgroup analysis, primary outcome measures including the Western Ontario and McMaster Universities OA index and subscales, timed walk, and secondary efficacy variables, including investigator global assessment for disease and global response to treatment, subject visual analog scale for discomfort, overall disease activity, global response to treatment, index joint tenderness and mobility, were evaluated for differing trends between the study groups. Results: Subset analyses revealed some statistically significant differences and some notable trends in favor of the flavocoxid group. These trends became stronger the longer the subjects continued on therapy. These observations were specifically noted in older subjects (>60 years), males and in subjects with milder disease, particularly those with lower subject global assessment of disease activity and investigator global assessment for disease and faster walking times at baseline. Initial analysis of the entire intent-to-treat population revealed that flavocoxid was as effective as naproxen in managing the signs and symptoms of OA of the knee. Detailed analyses of subject subsets demonstrated distinct trends in favor of flavocoxid for specific groups of subjects.
# Levy R, Khokhlov A, Kopenkin S, Bart B, Ermolova T, Kantemirova R, Mazurov V, Bell M, Caldron P, Pillai L, Burnett BP. Efficacy and safety of flavocoxid compared with naproxen in subjects with osteoarthritis of the knee—a subset analysis. Advances in Therapy. 2010; 27(12):1-10
Figure 1. Selected parameters grouped by investigator global assessment of disease <8.0 (less severe disease). Western Ontario and McMaster Universities osteoarthritis composite (WOMAC) index (6 and 12 weeks: P<0.0001); WOMAC pain (6 and 12 weeks: P<0.0001); WOMAC stiffness (6 weeks: P=0.15; 12 weeks: P=0.08); WOMAC physical function (6 weeks: P=0.04; 12 weeks: P=0.03). Asterisk indicates P<0.05.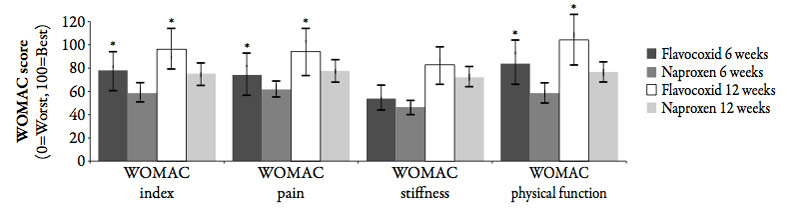
Open-label Phase IV post-marketing trial; the GOAL study £
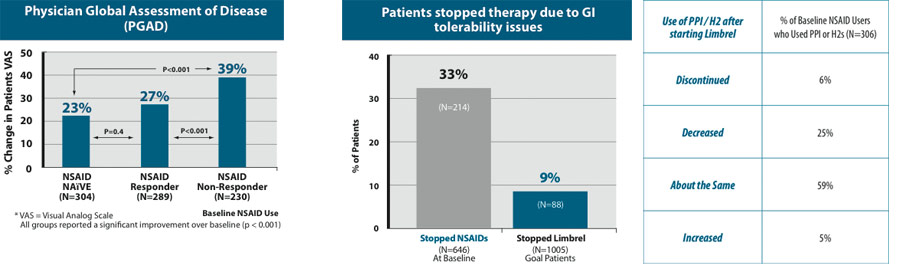
GOAL (Gauging OsteoArthritis with Limbrel), an open-label, post-marketing study, was performed to determine the overall efficacy and gastrointestinal (GI) tolerability of flavocoxid in a 'real world' clinical practice setting. To this end, the study enrolled several unique patient types including nonsteroidal anti-inflammatory drug (NSAID) naive patients, those who had used NSAIDs in the past, regardless of efficacy outcomes (positive or negative), those who showed good GI tolerance or intolerance to NSAIDs, and those who had previously taken a gastroprotective medication to improve GI tolerability or continued to take it as a precautionary measure to prevent NSAID-associated GI damage. A total of 1067 individuals at 41 rheumatology practices were enrolled and prescribed flavocoxid, 500 mg b.i.d., for 60 days. The Physician Global Assessment of Disease (PGAD) visual analog scale (VAS) was used as a global measure to assess the signs and symptoms of OA, including joint discomfort, stiffness, functional mobility and quality of life. In addition, overall tolerability and upper GI tolerability were assessed by individual questions scored on a 5-part Likert scale. The physicians also monitored any interruption in, or cessation of use of flavocoxid due to a GI issue as well as changes in the use of gastroprotective medications. Adverse event (AE) monitoring was also conducted. Of the 1005 patients who completed all follow-up visits, physicians recorded an average improvement in VAS scores from 60.1 (SD 18.8) at baseline to 42.5 (21.9) at 8 weeks (p=0.001) in 65.8% of patients. The PGAD VAS noted the most significant improvement in those patients with moderate to severe OA and in those patients who were historically non-responders to NSAIDs. Patients who had previously responded well to NSAIDs had VAS scores of 42.6 (19.8) vs. 58.0 (18.0) (p=0.001) and NSAID naive subjects showed improvement in VAS scores from 60.5 (18.0) at baseline to 46.3 (23.7) (p=0.001). The study recorded a low incidence (10%) of AEs reported to physicians and good overall tolerability to flavocoxid. Flavocoxid showed improved upper GI tolerability in almost 50% of previous NSAID users (p=0.001) and reduced therapy interruption in 90% of previous NSAID users with a history of GI-related therapy interruptions (p=0.0001). Finally, the use of flavocoxid resulted in a 31% reduction in or cessation of the use of gastroprotective medications (p=0.001).
Within a 'real world' clinical rheumatology practice setting, flavocoxid demonstrated significant efficacy in the management of OA in multiple patient types and displayed significant potential for reducing the possibility of adverse GI side-effects and use of gastroprotective agents associated with more traditional OA medications. Although the study was intentionally open-label and not rigorously controlled, the large population may compensate for this lack of control.
£ Pillai L, Burnett BP, Levy RM for the GOAL Study Cooperative Group. Open-label, post-marketing study of flavocoxid, a novel dual pathway inhibitor anti-inflammatory agent of botanical origin: the GOAL study. Current Medical Research and Opinion. 2010; 26(5):1055-1063
Special Populations
Effects on Platelet Aggregation Ω
Flavocoxid at a human equivalent dose (HED) of 569 mg was tested in a mouse model for its effect on platelet function. There was no significant increase or reduction of Ivy bleeding time and no potentiation of the effect of aspirin to prolong bleed times when flavocoxid was combined with aspirin at 370 mg HED (Pillai et al., 2010). Furthermore, healthy, human volunteers (n=10), given flavocoxid (500 mg BID) for 14 days, demonstrated no significant change in either AA-induced or spontaneous platelet aggregation or bleed times compared to baseline. There was also no difference in the baseline vs 14-day thromboxane levels in the flavocoxid-administered subjects. These results suggest that flavocoxid does not change thromboxane-induced platelet aggregation although it inhibits COX-1 peroxidase activity in vitro.
Ω Pillai L, Levy R, Yimam M, Zhao Y, Jia Q, Burnett BP. Flavoxocid, an anti-inflammatory agent of botanical origin, does not affect coagulation or interact with anticoagulation therapies. Advances in Therapy. 2010; 27(6):400-11
Effect of Limbrel on INR in warfarinized patients Ω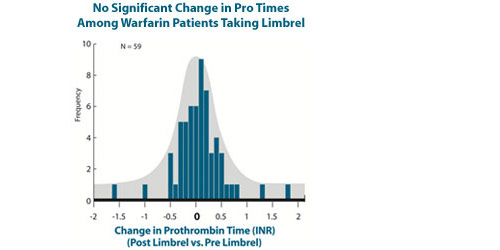
In an open-label trial, patients (n=59) currently taking Coumadin (warfarin) at various doses had their INRs evaluated before being placed on Limbrel. After 2 weeks of Limbrel therapy (either 250 or 500 mg bid), another INR was obtained. The results show that Limbrel does not appreciably affect INR. A few outliers with shortened as well as elongated INR were observed which may represent variations in the laboratory testing or inherited variations in the CYP450 enzyme system for metabolism of warfarin. The data are displayed as the number of standard deviations from average baseline value. None of the outlying values were sufficiently extreme as to put the patients a t risk for bleeding or clotting.
Ω Pillai L, Levy R, Yimam M, Zhao Y, Jia Q, Burnett BP. Flavoxocid, an anti-inflammatory agent of botanical origin, does not affect coagulation or interact with anticoagulation therapies. Advances in Therapy. 2010; 27(6):400-11
Additional Animal Models
Acute pancreatitis Δ
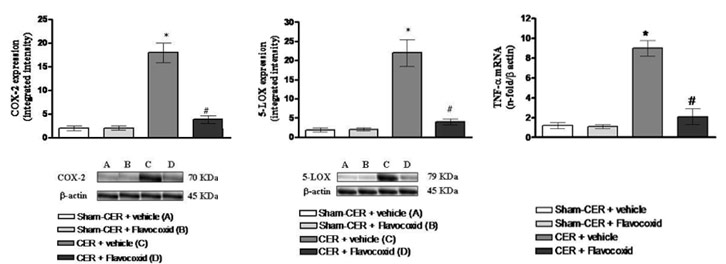
The ability of flavocoxid (Limbrel) to ameliorate experimental acute pancreatitis was studied in 28 male Sprague-Dawley rats given caerulein (CER; 80g/kg for each of four injections at hourly intervals) or vehicle (four intra-peritoneal injections of 0.9% saline). Animals were then randomized to receive flavocoxid (20 mg/kg i.p. administered 30 min. after the first injection of caerulein); or vehicle (a 10% DMSO/NaCl solution). Animals were killed 2 hours after the last caerulein injection to evaluate histological alterations; amylase, lipase, leukotriene B4 (LTB4) and prostaglandin E2 (PGE2) serum levels; COX-2 and 5-LOX expression and TNF-α gene expression by real time PCR. Flavocoxid inhibited COX-2 and 5-LOX activation, reduced serum lipase and amylase levels and the degree of edema, blunted the increased pancreatic TNF-α mRNA expression, LTB4 and PGE2 levels, and protected against the histological damage in terms of vacuolization and leukocyte infiltration. The data confirmed a key role for either COX-2 or 5-LOX in acute pancreatitis and suggested that flavocoxid might be a potential therapeutic approach to the treatment of patients at high risk of developing this life-threatening condition.
Δ Polito F, Bitto A, Irrera N, Letteria M, Fazzari C, Squadrito F, Altavilla D. Flavocoxid, a dual inhibitor of COX-2 and 5-LOX, reduces pancreatic damage in an experimental model of acute pancreatitis. Br J Pharmacol. 2010 November; 161(5):1002-11
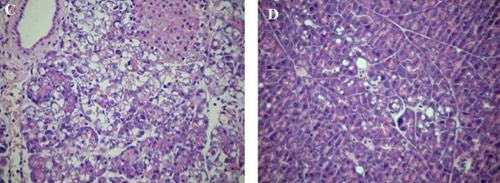
C:Cerulein
D: Cerulein+flavocoxid
This publication supports the antioxidant effects of flavocoxid as part of its mechanism of action in controlling inflammation.
Duchenne's muscular dystrophy (DMD) Σ
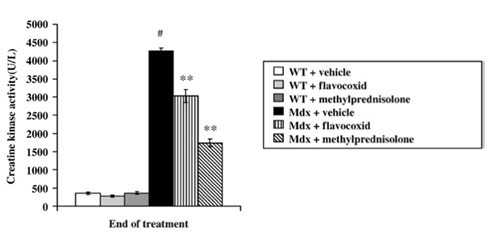 Nuclear factor(NF)-κB is known to be a key player in the pathogenesis of DMD. Because of its recognized inhibitory effects on this transcription factor, flavocoxid (Limbrel), having a potent antioxidant capacity, was investigated for its ability to suppress the inflammatory muscle lesion associated with DMD in the mdx mouse. A model for this disease and its effect was compared with prednisolone, the current standard of care. Five-week-old mdx mice were treated for 5 weeks with flavocoxid, methylprednisolone or vehicle. Serum samples were assayed for oxidative stress markers, creatine-kinase (CK) and leukotriene B-4. Cyclooxygenase-2 (COX-2), 5-lipoxygenase (5-LOX), tumor necrosis factor-α, p-38,JNK1 expression and NF-κB binding activity. The administration of flavocoxid: (1) ameliorated functional properties in vivo and ex vivo; (2) reduced CK; (3) reduced the expression of oxidative stress markers and of inflammatory mediators; (4) inhibited NF-κB and mitogen-activated protein kinases (MAPKs) signal pathways; (5) reduced muscle necrosis and enhanced regeneration. The results show that flavocoxid is as effective as prednisolone in the mdx mouse model of DMD.
Nuclear factor(NF)-κB is known to be a key player in the pathogenesis of DMD. Because of its recognized inhibitory effects on this transcription factor, flavocoxid (Limbrel), having a potent antioxidant capacity, was investigated for its ability to suppress the inflammatory muscle lesion associated with DMD in the mdx mouse. A model for this disease and its effect was compared with prednisolone, the current standard of care. Five-week-old mdx mice were treated for 5 weeks with flavocoxid, methylprednisolone or vehicle. Serum samples were assayed for oxidative stress markers, creatine-kinase (CK) and leukotriene B-4. Cyclooxygenase-2 (COX-2), 5-lipoxygenase (5-LOX), tumor necrosis factor-α, p-38,JNK1 expression and NF-κB binding activity. The administration of flavocoxid: (1) ameliorated functional properties in vivo and ex vivo; (2) reduced CK; (3) reduced the expression of oxidative stress markers and of inflammatory mediators; (4) inhibited NF-κB and mitogen-activated protein kinases (MAPKs) signal pathways; (5) reduced muscle necrosis and enhanced regeneration. The results show that flavocoxid is as effective as prednisolone in the mdx mouse model of DMD.
Σ Messina S, Bitto A, Aguennouz M, Mazzeo A, Migliorato A, Polito F, Irrera N, Altavilla D, Luca Vita G, Russo M, Naro A, Grazia De Pasquale M, Rizzuto E, Musarò A, Squadrito F, Vita G. Flavocoxid counteracts muscle necrosis and improves functional properties in mdx mice: a comparison study with methylprednisolone. Experimental Neurology 220. 2009; 349-358
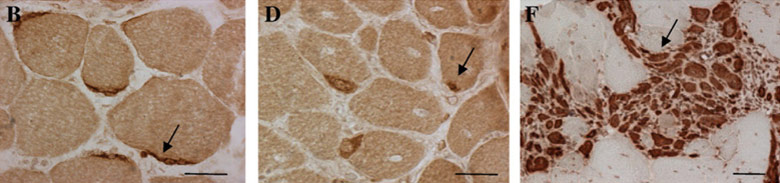
B: Flavocoxid
D:Prednisolone
F: Vehicle
This data again backs up the antioxidant effects of flavocoxid on the management of inflammation. Well-controlled clinical trials using endpoints which measure oxidative status as well as antioxidant influenced markers need to be performed in humans.
New and Ongoing Clinical Studies
Various randomized, double-blind, placebo-controlled clinical trials of large sample sizes including mild and moderate osteoarthritis patients are underway by independent investigators.
These new and ongoing clinical studies will provide further long term safety and effectiveness results for Limbrel versus other marketed osteoarthritis products. All studies have been IRB approved.
Long-term Clinical Experience
The constituent ingredients in Limbrel have been extensively studied individually and are available as prescription medical products in numerous countries around the world(17). For example, in Japan, which has exceedingly rigorous standards for prescription products, the primary constituent ingredients of Limbrel have been available in prescription anti-inflammatory products and reimbursed by Japan's national health insurance for decades. Both Scutellaria baicalensis and Acacia catechu are listed in the Official Japanese Pharmacopoeia(18). Finally, millions have safely consumed the extracts of these plants as traditional medicines worldwide for generations.